

Who Is an Ideal Candidate for Cochlear Implant Surgery?
March 13, 2026
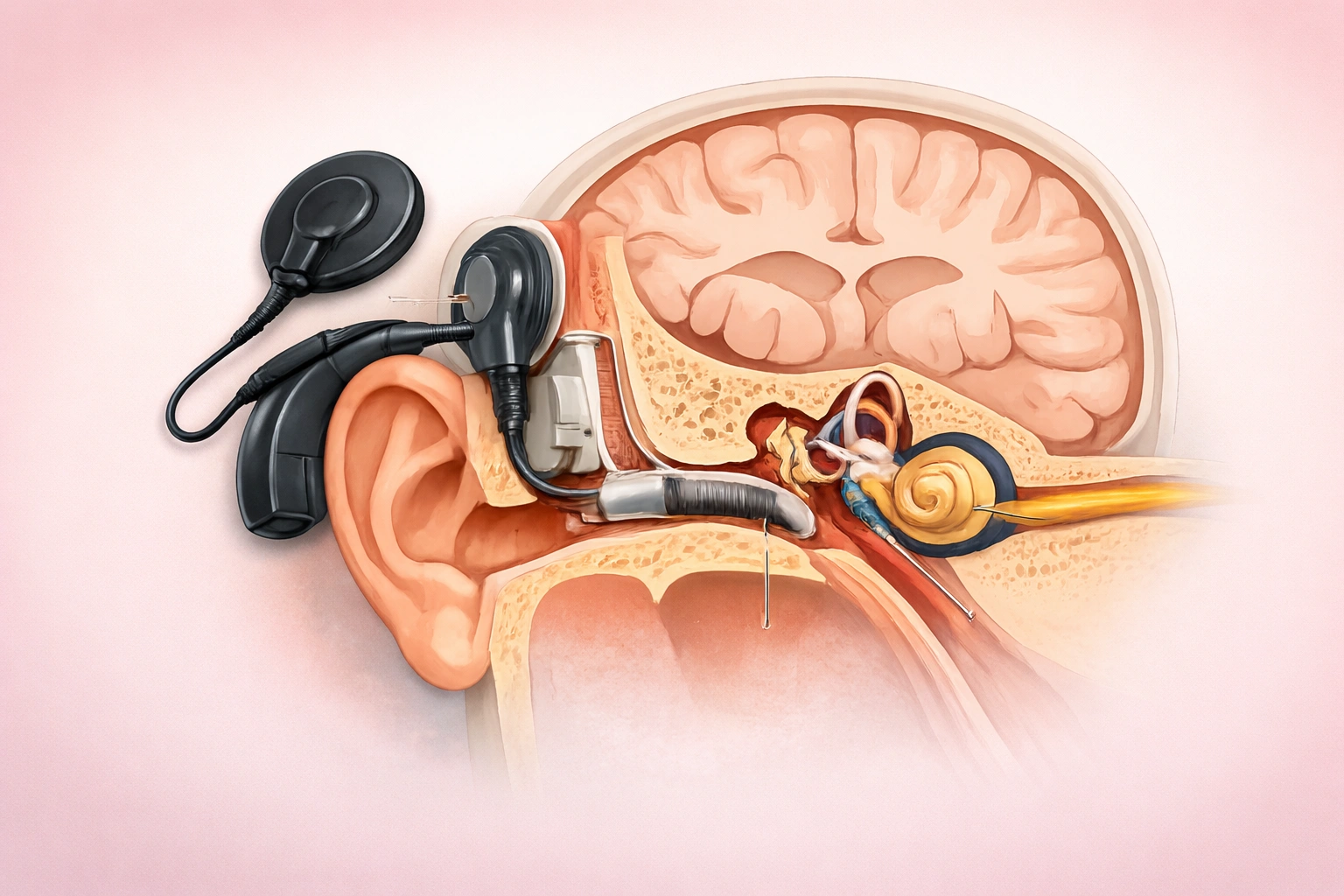
A cochlear implant functions unlike a hearing aid in every way. Where one merely increases volume, the other routes signals past injured parts of the inner ear straight to the hearing nerve. Sound perception now reaches people once surrounded by complete quiet, thanks to advances emerging around 2026. Yet surgery requiring implanted components limits eligibility - some forms of deafness do not qualify. Only when selection guidelines are clearly recognized does outcome predictability improve.
People With Very Little or No Ability to Hear Sounds
Individuals considered first for cochlear implants often have deep hearing impairment in both ears due to nerve-related causes. Originating within the inner ear, this condition usually stems from harm to microscopic sensory cells inside the cochlea - structures essential for relaying noise information toward the central nervous system. In cases where such cells no longer exist or function poorly, amplification devices - even advanced ones - fail to deliver intelligible spoken language. Hearing noises without recognizing speech clearly, despite using premium-grade assistive equipment, might indicate a need for artificial signal transmission through implanted technology.
Limited Help from Standard Hearing Aids
Only after standard hearing devices fail to provide benefit should surgical options be considered. Testing often involves listening tasks conducted by specialists while using properly adjusted equipment. Should results reveal minimal comprehension even in quiet settings, this suggests the ear’s ability to process sound is severely limited. When typical support systems deliver little meaningful improvement, further intervention may become necessary. Communication difficulties during routine interactions frequently mark the point at which alternative solutions emerge as relevant.
The Role of Systemic Health and Fluid Balance
Stability in bodily functions matters greatly when preparing for cochlear implantation, since general anesthesia demands consistent internal conditions. Electrolytes and fluids stay balanced largely due to kidney activity - this balance directly affects the inner ear's surroundings. When fluid control falters, swelling or excess pressure may develop, possibly disrupting how well the implanted electrodes settle into place. In children, or individuals with past kidney concerns, advice from a specialist in urinary health often brings clarity before proceeding. Ensuring harmony within these systems becomes one fixed point on the path toward readiness for the procedure.
Protecting the Sensory Foundation
Under the skin behind the ear lies where the internal processor goes, needing sound tissue to heal well. Resilience in that skin matters - chronic irritation must be absent. Protection of the outer layer before and after surgery avoids complications while supporting how the external part rests. Stability begins with sensation; when the scalp feels balanced, adaptation follows more smoothly. Long-term function ties closely to early care around the implant site.
After Surgery Care and Recovery
What makes someone well-suited includes deep psychological readiness alongside active participation in recovery. Rather than delivering instant natural sound, a cochlear implant introduces electrical impulses requiring adaptation. Over time, through repeated practice, the mind learns to recognize these unfamiliar patterns. Progress depends on ongoing sessions focused on listening skills and spoken language, maintained across many weeks. Candidates showing high motivation often succeed when steady encouragement exists within their living environment. Achievement follows not only the operation, but also what happens afterward. What occurs beyond the operating room holds equal weight. Progress depends on consistent effort made long after medical intervention ends.
Anatomical Fit for the Implant
Ultimately, the ear's anatomy needs to support implant placement. To check this, medical staff rely on CT and MRI images, looking specifically at whether the cochlea shows signs of hardening or if the hearing nerve remains whole. In cases where the route for the electrode faces obstruction, or when the nerve fails to transmit impulses, the device will not work as intended. Such scanning methods form a routine element of assessment, verifying that installation of the component can proceed without risk and with reasonable chance of function.
Conclusion
Cochlear implant surgery offers support when standard hearing aids do not help. Should healing include attention to skin integrity, while also reviewing bodily fluid levels under guidance from a pediatric urologist, overall health management becomes more complete. Meeting medical guidelines along with engaging in listening exercises allows access to improved sound awareness. When current devices fail to deliver clear hearing, discussion with a doctor focused on ear conditions may lead toward considering this method.